A) K wire fixation
B) Open reduction and internal fixation
C) Cuff and sling only
D) Manual reduction and slab application
Ans: B
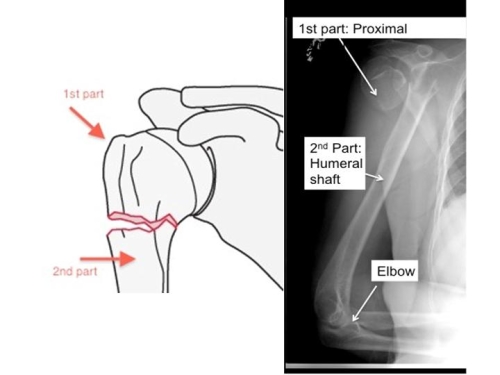
In the Neer Classification of proximal humerus fracture, the head of the humerus is made up of 4 parts:
1) Humeral head (articular surface)
2) Greater tubercle
3) Lesser tubercle
4) Diaphysis (shaft) by epiphyseal lines
These four parts are separated by epiphysial lines (bony growth plates) during th early developmental years. When he proximal humerus is broken, the fracture line predictably occurs along one or more of these places.
In general, 2 or 3 part fractures are treaed with open reduction and internal fixation. A plate with screws is the choice of many surgeons currently.
Four part fractures in the younger, active patient also can be treated successfully with open reduction and internal fixation. However in the elderly and in patients with osteoporosis a hemiarthroplasty is the treatment of choice.
 |
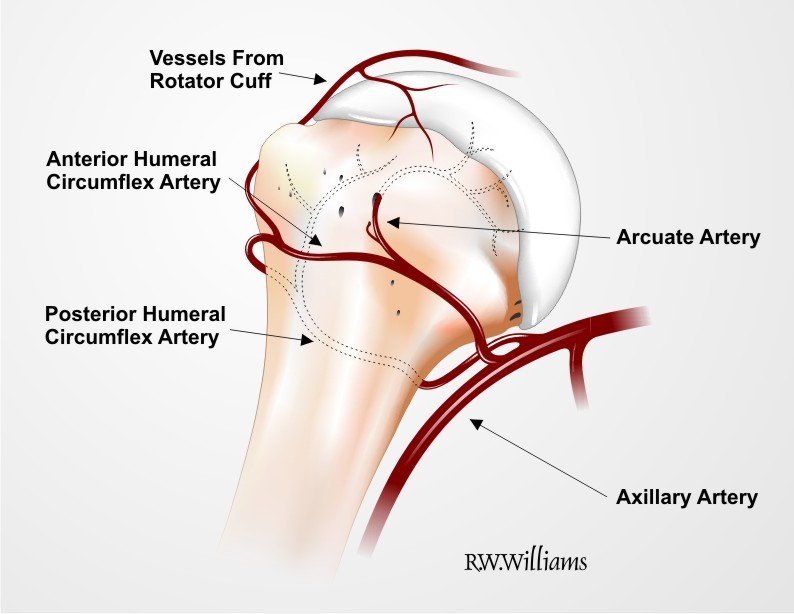
| Parts of proximal humerus: articular head, Greater tuberosity and Lesser tuberosity for insertion of rotator cuff, metaphyseal flare, surgical neck, anatomical neck. Inclination of the humeral head relative to the shaft averages 130 degrees Humeral retroversion 18-40 degrees. Bone density of subchondral bone is strongest. |
Proximal humerus is formed by 3 ossification centres. Fusion of these ossification centres at the physis creates a weakened area that is susceptible to fracture. Primary deforming forces- pectoralis major and rotator cuff. Blood supply is by distal branches of axillary artery
Arcuate artery of Liang- supplies humeral head.
Tethered trifurcation- at the level of surgical neck- vascular injury
Proximal Humerus fracture
2-4% of upper extremity fracture. Accounts for 5% of all fractures and is the second most common fracture of the upper limb.
Majority occur in the elderly (>65). It is usually minimally displaced and stable/ Osteoporotic and metaphyseal fractures with compromised bone quality- optimal surgical and functional outcomes are limited.
Females are affected 3 times more often than males.
How it happens: in younger age group= high energy trauma eg MVA or indirectly by seizures and electric shock.
In older age group= low energy trauma, eg fall on outstretched hand.
Most are non displaced and have good prognosis and does not need any surgery
Risk factors
Elderly
Osteoporotic
Impaired vision
Balance
Medical comorbidities
Decreased muscle tone
Aim of management
Irrespective of age, operative or non operative management is aimed to achieve a stable pain free range of movement of the limb, thereby avoiding the late sequelae like refractory shoulder, stiffness, osteonecrosis, malunion, nonunion and heterotopic calcification.
In order to achieve this, it is imperative to pay utmost attention to the anatomical distortion and disturbance of the shoulder joint that is inherent ot he proximal humeral fracture.
At this juncture it is pertinent to look at the anatomical profile of the proximal humerus, which has a direct bearing on the diagnosis, workup, treatment protocols and rehabilitation.
What to note:
Number of fracture parts
Displacement per part.
- One part fracture: fracture lines involve 1-4 parts. None of the parts are dispaced (ie <1cm and <45 degrees.




- Two part fracture (20%): fracture line involves 2-4 parts. One part is displaced
- Surgical neck: most common
- Greater tuberosity: frequently seen in the setting of anterior shoulder dislocation and has a lower threshold of dislocation
- Anatomical neck
- Lesser tuberosity (uncommon)

 |
| two part lesser tuberosity |
 |
| A: two part surgical neck fracture B: after treatment with closed reduction and percutaneous pinning |
 |
| 2 part fracture of the surgical neck with subsequent internal fixation |
Two part Fracture (Avulsion Fracture)
Most commonly occur as a result of seizures or secondary to glenohumeral dislocations. THese often reduce anatomically with reduction of the humeral head and can be managed nonoperatively. Displaced more than 1cm, open reduction and internal fixation are required.
Fixation with screws, wire, or suture as dictated by the size of the fragment, the comminution or quality of the bone. If tuberosity has been displaced and retracted a significant tear in the rotator cough mechanism exists also. Careful identification and repair of the rotator cuff defect are required.
- Three part fracture: fracture lines involve 3-4 parts and 3 parts are displaced with respect to the 4th part. Uncommon (<1%). As the articular surface is no longer attached to any parts of the humerus which are attached to soft tissues it has a high incidence of osteonecrosis and poor non operative results.
 |
| True AP radiograph of a head splitting three part proximal humeral fracture in a 70 year old woman Postoperative radiograph after humeral head replacement |
Four Part Fracture:
Clinical Evaluation
Ecchymosis appears 24-48 hours later.
Look also for rib, scapular and cervical # in high energy trauma.
Concurrent brachial plexus injury in 5%
Axillary nerve is susceptible in anterior fracture dislocation
Gentle rotation of arm and palpation of #- guide for # stability
Diagnosis
Scapular AP, Y - lateral, abducted and Velpeau axillary view
CT- to assess glenoid #, dislocation, comminution and posteriorly displaced GT or medially displaced LT fragments
MRI: Patient had preinjury shoulder problem (cuff tear), pathological #, nonunion
There are different classification systems for proximal fracture of the humerus:
Edwin smith papyrus- open vs closed
Kocher: location of #, supratubercular, periT, infraT, subT
Codman: 11 different types, described # along the lines of epiphyseal scars
Watson and Jones: based on mechanism of injury
AO: 27 possible subgroups, emphasizes on vascular supply of articular portion of PH
DePalma and Cautili emphasized the difference between fracture with and without dislocation of the joint surfaces
Neer classification: # classified by evaluating the displacement of parts from each other. Criteria to consider as a part, fragment must be rotated 45 degrees or 1cm from the another fragment.
This one is commonly used because it is based on the regional anatomy and emphasis on degree of displacement.
Impacted Fractures
Almost exclusively in older people
Tend to develop periarthritis about the shoulder, these fractures shoulder be treated by methods that allow early motion and early restoration of function
Treatment
Most fractures (>80%) can be treated conservatively
Indication:
Non displaced #: <5mm of superior 10mm of posterior GT displacement in active patients and <10mm of superior displacement in nondominant arm in sedentary patient
Surgical neck #: any bone contact in elederly patient, in young patient <50% shaft diameter displacemet and <45 degrees angulation in dominant arm
Reduced demand: patient willing to accept stiffness
Poor health: patient unable to tolerate surgery and anaesthesia
Poor rehabilitation candidate
Minimally Displaced Fracture
Fracture of Greater Tuberosity
Undisplaced and comminuted. Sometimes it is widely separated due to pull by the muscle (supraspinatus) attached to it.
Principle: early protection and combined with gradual mobilisation
Early triangular sling immobilisation for 7-10 days
Active finger, wrist, elbow movements
By 2 weeks, gentle active assisted ROM exercises
By 6 weeks, light resistive exercises
By 3 months, shoulder strengthening
Two part fracture
Involving the anatomical neck: articular fragment is rendered avascular and may require prosthetic replacement.
Involving the surgical neck usually can be treated by a sling hanging arm cast or other conservative measures
Indications for operative treatment:
- Open fractures
- Inability to obtain or maintain an acceptable closed reduction
- injury to the axillary artery
- selected multiple trauma patients
Types: Percutaneous treatment vs Open reduction internal fixation
When to do closed reduction percutaneous fixation:
- Fracture without significant comminution in patient with good quality bone
- Patient should be willing to comply with postop care plan
When not to do percutaneous fixation
- Severe comminution
- Osteopenia
- Inability to reduce the fracture
ORIF
Iinternal fixation with a combination of intramedullary rod fixation and tension band technique or intramedullary rod fixation with a proximal locking screw.
A hand-bent semitubular plate used as a blade plate device also is satisfactory in osteopenic bone
In younger patients, an AO buttress plate with screws also is useful
Three Part fracture
ORIF
When to do humeral head replacement?
When injury has caused avascularity of articular segment which even with a satisfactory reduction and fixation would eventually collapse- post-traumatic arthritis
- Four part fracture and fracture dislocations
- Three part fracture and fracture dislocations in elderly patients with osteopenic bone, anatomic neck
- Head splitting fracture
- Anatomic neck fracture that can not be reduced and fixed
- Chronic dislocation with impression fracture involving >40% articular surface.
COMPLICATIONS
More likely after surgical than nonoperative fracture care
1) Instability: due to glenoid fracture, rotator cuff tear or muscle atony
Rx: ORIF glenoid, repair of the cuff, isometric exercises
2) Malunion: due to incorrect diagnosis, poor reduction, inadequate fixation
Rx: Release of adhesions, with or without osteotomy. Or more simply, trim off the prominence
3) Nonunion: Motion too early poor bone. Preserved head- ORIF and BG
Cavitated head- HHR
4) Avascular necrosis: four part fracture and dislocation. HHR
5) Neurovascular injury: Four part with head in axilla. If nerve injury + at the time of closed injury, prognosis is good
6) Infection: Immune compromise and extensive soft tissue loss. Hardware removal and debridement
7) Arthritis: Hardware penetrating the joint. Refractory shoulder stiffness
8) Charcot shoulder: Unusual fragmentation occurs after fracture
9) Heterotopic bone formation: Soft tissue injury, repeated manipaulation, delayed reduction beyond 7 days/
No comments:
Post a Comment